
AI-Powered Meal Scanning and Insulin Calculation: How Mobile Apps Are Changing Diabetes Management
From handwritten food diaries to real-time AI analysis, the tools available for diabetes self-management have undergone a fundamental transformation. This article examines the technology, market evidence, and design principles behind AI-powered meal scanning — and why the next generation of apps must go beyond calorie counting to serve the insulin-using community.
1. The Evolution of Diabetes Self-Management
For decades, the standard of care for people with diabetes involved a pen, a paper logbook, and a food composition table. Patients manually estimated carbohydrate content of meals, recorded blood glucose readings from finger-prick tests, and brought spiral-bound notebooks to quarterly endocrinologist visits. The data was fragmented, retrospective, and difficult to act upon in the moment that mattered — before eating.
The first wave of digital tools (roughly 2008–2015) replaced paper with smartphone apps like mySugr and Glucose Buddy. They digitized the logbook but preserved its fundamental limitation: manual text entry of food items. A 2017 systematic review published in the Journal of Medical Internet Research found that while diabetes apps improved HbA1c by an average of 0.4% compared to usual care, adherence to manual food logging declined sharply after 10–14 days [1].
The second wave (2016–2022) introduced barcode scanning and integration with continuous glucose monitors (CGMs). Apps like Libre LinkUp and Dexcom Clarity enabled real-time glucose streaming, but the meal side of the equation — the most labor-intensive and error-prone component — remained manual.
The third wave, now emerging, applies computer vision and large language models to automate the meal-logging step entirely. A user photographs their plate, and the system returns a nutritional estimate in seconds. This shift from recall-based logging to perception-based scanning removes the primary friction point that has limited adherence for two decades.
2. How AI Food Recognition Works: The Photo-to-Carbs Pipeline
Modern AI food recognition is not a single model — it is a multi-stage pipeline that combines computer vision, natural language understanding, and nutritional databases. The process operates in four sequential phases:
Phase 1: Image Capture & Preprocessing
The user captures a photograph of their meal. The system preprocesses the image — normalizing lighting conditions, applying perspective correction, and segmenting individual food items on the plate using instance segmentation models (e.g., Mask R-CNN or SAM-based architectures). Multi-item plates are decomposed into individual regions of interest.
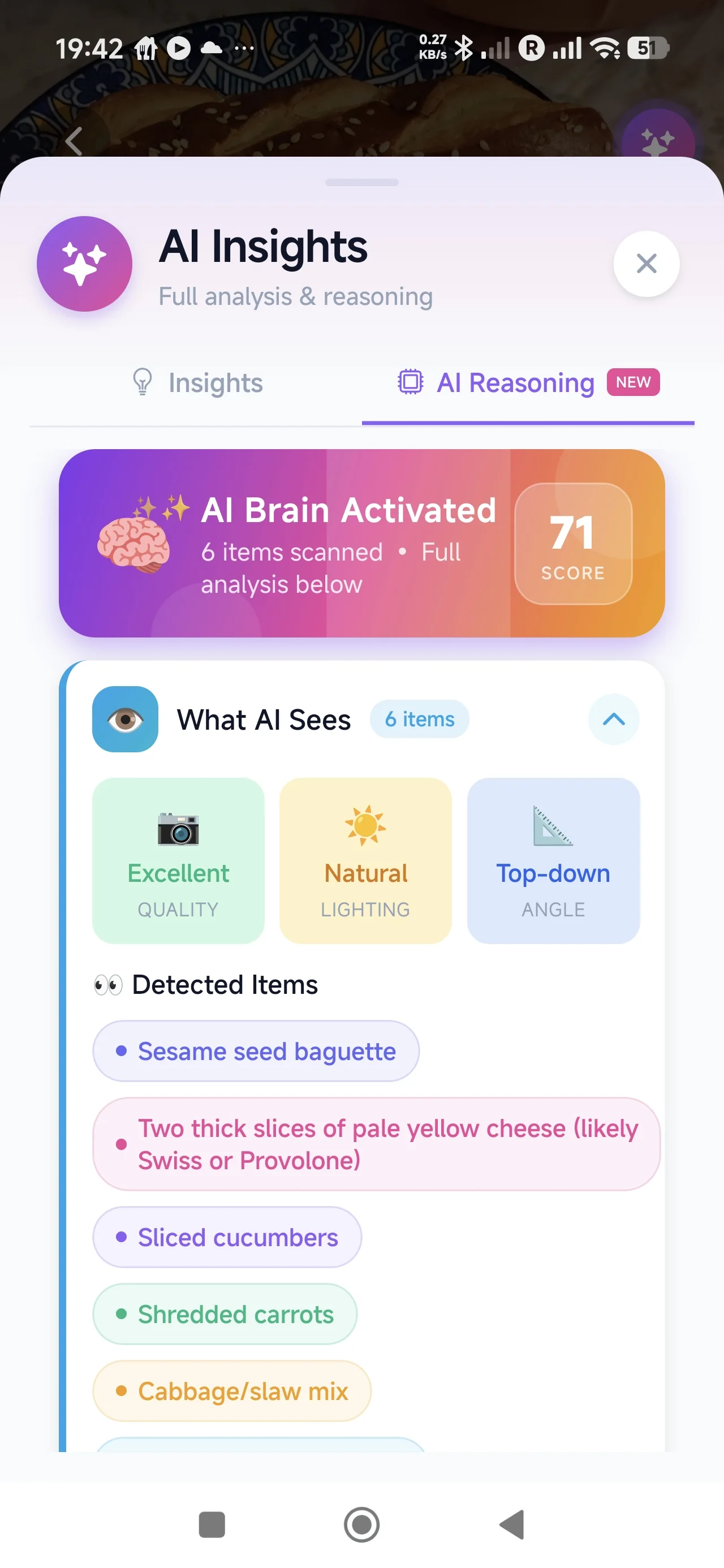
Phase 2: Food Classification
Each segmented region is passed through a convolutional neural network (CNN) or vision transformer trained on large-scale food image datasets. Models such as Google’s Food-101 or proprietary datasets with 100,000+ labeled food categories classify each item. Modern systems increasingly use multimodal models (GPT-4V, Gemini Vision) that accept an image and return structured food identification with portion estimation in natural language [2].
Phase 3: Nutrition Database Lookup
Identified food items are mapped against verified nutritional databases — USDA FoodData Central, national composition tables, or proprietary datasets. The system retrieves macronutrient profiles: total carbohydrates, fiber, fat, protein, and glycemic index where available. Portion size estimation uses depth cues, reference objects, or learned priors from training data.
Phase 4: Carbohydrate Estimation & Confidence Scoring
The pipeline outputs a total carbohydrate estimate with a confidence interval. High-confidence items (packaged foods, common dishes) return tight estimates; complex or unfamiliar items flag wider ranges for user review. A 2023 study in Nutrients found that AI-based carb estimation achieved a mean absolute error of 10–15 grams per meal, comparable to trained dietitians [3].
3. Market Validation: Proof That Users Want AI Food Scanning
The commercial evidence for AI-powered food scanning is no longer speculative — it is demonstrated at scale. Several companies have validated the core user behavior of photographing meals for nutritional insight:
- Cal AI reached $30 million in annual recurring revenue and surpassed 10 million users within 18 months of launch, growing primarily through organic word-of-mouth and social media virality. Their value proposition is radically simple: take a photo, get calories [4].
- YAZIO, a European nutrition tracker, generates approximately $2 million per month in subscription revenue and has consistently ranked in the top 10 health & fitness apps globally. Their integration of AI photo scanning significantly improved conversion from free to premium tiers.
- Foodvisor and Bitesnap have each processed hundreds of millions of meal photos, validating that the core user action — point, shoot, log — eliminates the adherence cliff that plagues text-based food logging.
These numbers demonstrate unambiguous demand. However, every one of these successful products targets the general wellness and weight-management market. Their output is calories. For the 537 million adults worldwide living with diabetes [5], the relevant output is not calories — it is carbohydrates, and specifically, carbohydrates in a form that can inform insulin dosing decisions.
4. Type 1 vs. Type 2: Different Needs From the Same Technology
While AI meal scanning serves both populations, the clinical workflow differs substantially:
Type 1 Diabetes (T1D)
People with Type 1 diabetes produce no endogenous insulin and must calculate a bolus dose for every meal. The standard formula is: Bolus = (Carbs ÷ ICR) + (Current BG − Target BG) ÷ ISF, where ICR is the insulin-to-carb ratio and ISF is the insulin sensitivity factor. For this population, carbohydrate estimation accuracy directly impacts glycemic outcomes. A 10-gram carb estimation error in a person with an ICR of 1:10 translates to a 1-unit dosing discrepancy — clinically meaningful for tight control [6].
The primary value of AI scanning for T1D is speed and reduced cognitive burden. Carb counting is a skill that requires years to develop and degrades under fatigue, distraction, and unfamiliar cuisines. Automating estimation reduces decision fatigue at every meal.
Type 2 Diabetes (T2D)
The majority of people with Type 2 diabetes manage their condition through lifestyle modification, oral medications, or basal insulin without meal-time bolusing. For this population, the primary need is portion awareness and pattern recognition — understanding which meals reliably spike glucose and which do not.
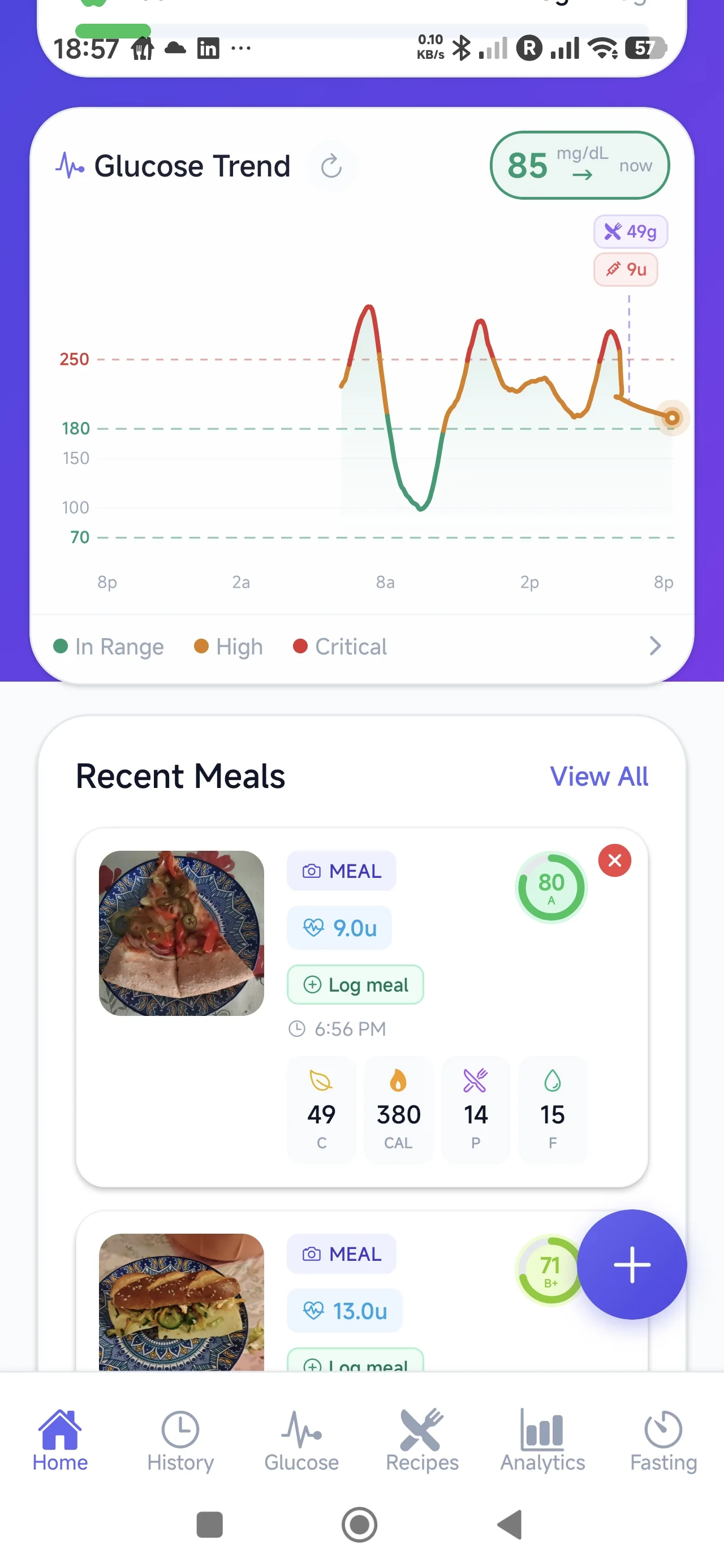
AI scanning serves T2D users by making food logging effortless enough to sustain. When combined with CGM data, even simple pattern recognition (“your post-meal glucose exceeded 180 mg/dL after rice-based meals on 4 of 5 occasions this week”) becomes actionable without requiring bolus calculation.
5. The Gap Most Food-Scanning Apps Miss
Existing AI food-scanning applications stop at the point of nutritional output. They answer the question “what did I eat?” but not the questions that matter for diabetes management: “how should this meal inform my insulin decision?” and “what actually happened to my glucose after this meal?”
This gap exists because general-purpose nutrition apps are built for a weight-management user journey. Their feedback loop is: log meal → see calories → compare to daily budget. The diabetes feedback loop is fundamentally different: estimate carbs → review insulin context → eat → observe glucose response → learn for next time.
The critical missing link is the connection between the meal and what happens next. Without linking meal data to insulin context and post-meal glucose response, each meal exists as an isolated event rather than a data point in a learning system. A food scanner that does not close this loop provides information without insight.
Key insight: For insulin-using diabetics, a food scanner is only useful if it participates in the insulin decision workflow — not as a dosing engine, but as a contextual support tool that reduces cognitive load at the moment of decision.
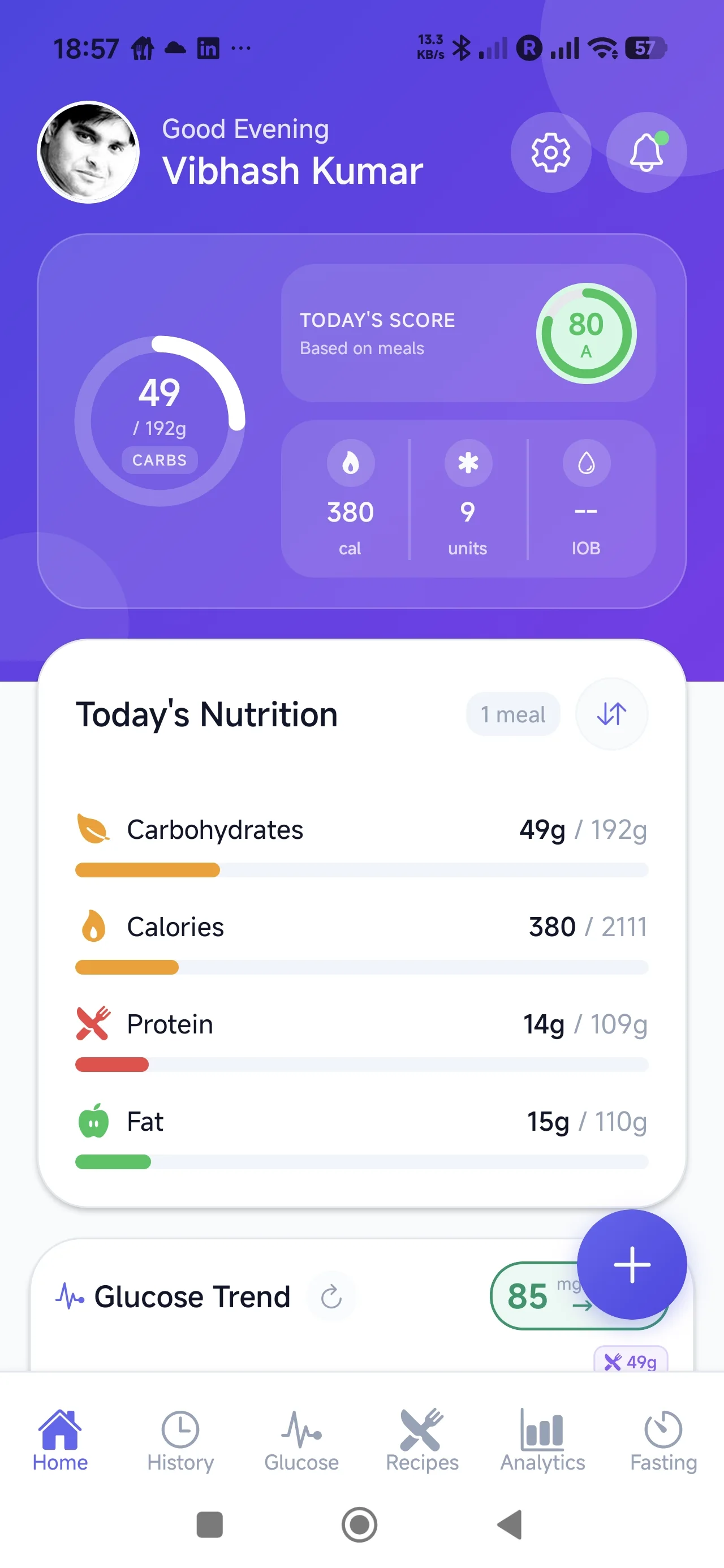
6. How GlucIQ Bridges the Gap: From Scan to Learning
GlucIQ is designed specifically for the diabetes feedback loop. Rather than treating meal scanning as an endpoint, it positions the scan as the first step in a four-phase workflow:
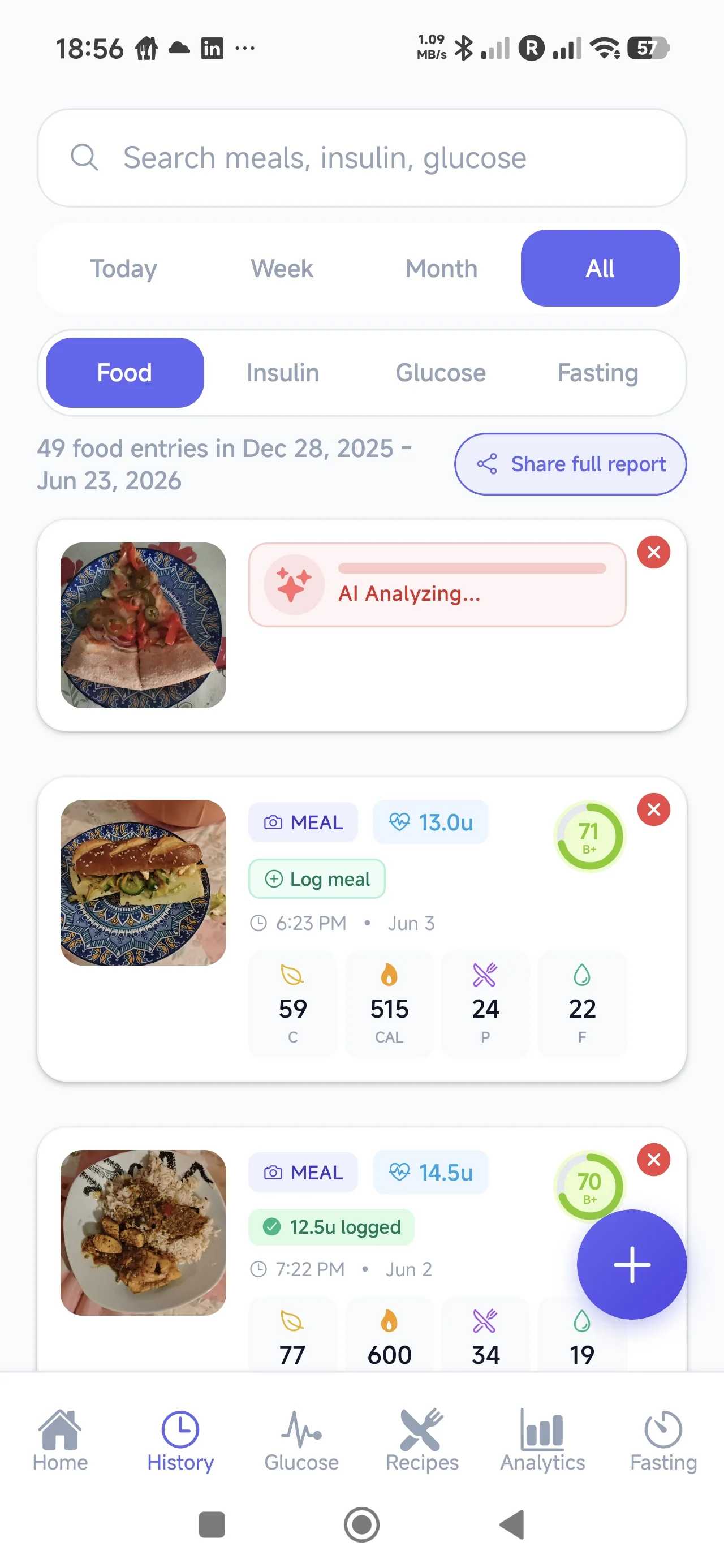
Step 1: Meal Scan
The user photographs their meal. GlucIQ’s AI identifies food items, estimates carbohydrate content, and presents results for user confirmation or adjustment. The interface is designed for speed — the goal is under 10 seconds from camera to confirmed estimate.
Step 2: Insulin Context Review
GlucIQ presents the carbohydrate estimate alongside the user’s personal insulin parameters (ICR, ISF, target glucose) so they can review the mathematical context for their dosing decision. The app does not prescribe or automate doses — it surfaces the relevant numbers in a clear, readable format so the user can make an informed decision with their healthcare provider’s guidance.
Step 3: Glucose Response Observation
After the meal, GlucIQ tracks the post-prandial glucose curve (via CGM integration or manual entries). The meal, insulin context, and glucose response are linked as a single event — creating a complete record of cause and effect.
Step 4: Pattern Learning
Over time, GlucIQ identifies patterns: meals that consistently produce favorable glucose responses, meals that don’t, and correlations between estimation accuracy and outcomes. These insights are delivered as periodic summaries — supporting the user’s growing understanding of their personal glucose dynamics.
Important distinction: GlucIQ is a support tool for self-management education and review. It does not replace clinical judgment, automate insulin delivery, or prescribe treatment. All insulin dosing decisions remain with the user in consultation with their healthcare team.
7. The Importance of Emotional Design in Diabetes Technology
Diabetes imposes a continuous cognitive and emotional burden. Every meal is a math problem. Every glucose reading carries implicit judgment — the language of “good” and “bad” numbers pervades the lived experience. Research consistently shows elevated rates of diabetes distress, with 18–45% of people with diabetes reporting significant emotional burden related to self-management [7].
Technology that adds complexity or generates anxiety — through aggressive alerts, punitive language, or overwhelming data density — risks exacerbating this burden. The most effective health technology companies have recognized that emotional design is not a cosmetic concern; it is a clinical one.
Headspace and Calm demonstrated that meditation apps succeed when they reduce perceived effort. Noom showed that behavior change scales when the interface feels supportive rather than prescriptive. Oura Ring proved that health data can be presented as curiosity rather than obligation.
GlucIQ applies these principles deliberately. The visual language uses calm gradients rather than alarm-red warnings. Glucose data is presented as a narrative (“here’s what happened”) rather than a verdict (“you failed”). Insights are framed as discoveries (“you might notice…”) rather than directives (“you should…”). The goal is an app that a person with diabetes wants to open, not one they feel obligated to use.
This design philosophy is grounded in Self-Determination Theory: sustained engagement requires that technology support autonomy (user retains control), competence (insights build confidence over time), and relatedness (the tool feels like an ally, not a monitor) [8].
8. Clinical Context: Standards of Care and Supporting Evidence
The American Diabetes Association’s 2024 Standards of Care explicitly recommend technology-assisted self-management for people with diabetes. Section 7 (“Diabetes Technology”) states that “the use of technology should be individualized based on a person’s needs, desires, skill level, and availability of devices” and endorses CGM use across all insulin-treated diabetes types [9].
The clinical evidence supporting combined CGM and meal logging is substantial:
- A 2022 randomized controlled trial in Diabetes Care demonstrated that CGM users who also logged meals achieved 12% greater time-in-range (70–180 mg/dL) compared to CGM-only users over 6 months [10].
- The landmark REPLACE-BG trial established that CGM-based glucose data, when combined with structured self-management education, reduces hypoglycemia without increasing HbA1c [11].
- A 2023 meta-analysis in The Lancet Digital Health found that AI-assisted diabetes management tools improved HbA1c by 0.3–0.6% and improved time-in-range by 8–14 percentage points compared to standard care, with the largest effects seen in tools that combined multiple data streams (CGM + meal + insulin) [12].
The convergence of affordable CGMs (Libre 3, Dexcom G7), mature AI food recognition, and smartphone ubiquity creates the conditions for a new category of diabetes tools that integrate all three data streams into a coherent self-management experience.
9. Medical Disclaimer
GlucIQ is a self-management support tool designed to assist people with diabetes in tracking meals, reviewing insulin calculation context, and observing glucose patterns. It is not a medical device, does not provide medical advice, and does not automate or prescribe insulin doses. The carbohydrate estimates provided by AI food recognition are approximations and should be verified by the user. All treatment decisions — including insulin dosing — must be made by the individual in consultation with their qualified healthcare provider. GlucIQ does not replace professional medical guidance, continuous glucose monitor clinical alerts, or insulin pump automated delivery systems. Users should always follow the treatment plan established with their diabetes care team.
Conclusion
AI-powered meal scanning has been validated at scale in the general wellness market. The technology works. The user behavior — photographing meals for instant feedback — is natural and sustainable. But for the hundreds of millions of people managing diabetes, particularly those using insulin, the current generation of food-scanning apps stops too early in the workflow.
The opportunity is not to build another calorie counter with a diabetes label. It is to build a purpose-designed tool that uses AI meal scanning as the entry point to a complete feedback loop: scan, review insulin context, observe glucose response, and learn from patterns over time. This is the system that GlucIQ is building — calm, intelligent, and designed around the actual decision architecture of life with diabetes.
References
- Hou C, Carter B, Hewitt J, Francesca T, Mayor S. Do mobile phone applications improve glycemic control (HbA1c) in the self-management of diabetes? A systematic review, meta-analysis, and GRADE of 14 randomized trials. Diabetes Care. 2016;39(11):2089-2095. doi:10.2337/dc16-0346
- Thames Q, Karber A, Rosenthal G, et al. Nutrition5k: Towards automatic nutritional understanding of generic food. Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition. 2021:8903-8911.
- Lu Y, Stathopoulou T, Vasiloglou MF, et al. An artificial intelligence-based system for nutrient intake assessment of hospitalised patients. Nutrients. 2023;15(18):4013. doi:10.3390/nu15184013
- Cal AI company metrics reported via Appfigures and Sensor Tower market intelligence, Q1 2025.
- International Diabetes Federation. IDF Diabetes Atlas, 10th edition. Brussels, Belgium: International Diabetes Federation; 2021.
- Bell KJ, Barclay AW, Petocz P, Colagiuri S, Brand-Miller JC. Efficacy of carbohydrate counting in type 1 diabetes: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2014;2(2):133-140. doi:10.1016/S2213-8587(13)70144-X
- Perrin NE, Davies MJ, Robertson N, Snoek FJ, Khunti K. The prevalence of diabetes-specific emotional distress in people with Type 2 diabetes: a systematic review and meta-analysis. Diabet Med. 2017;34(11):1508-1520. doi:10.1111/dme.13448
- Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68-78. doi:10.1037/0003-066X.55.1.68
- American Diabetes Association Professional Practice Committee. Standards of Care in Diabetes — 2024. Diabetes Care. 2024;47(Supplement_1):S1-S321. doi:10.2337/dc24-SINT
- Reddy M, Jugnee N, El Laboudi A, Spanudakis E, Anantharaja S, Oliver N. A randomized controlled pilot study of continuous glucose monitoring and flash glucose monitoring in people with Type 1 diabetes and impaired awareness of hypoglycaemia. Diabetes Care. 2018;41(3):483-490. doi:10.2337/dc17-1477
- Aleppo G, Ruedy KJ, Riddlesworth TD, et al. REPLACE-BG: a randomized trial comparing continuous glucose monitoring with and without routine blood glucose monitoring in adults with well-controlled type 1 diabetes. Diabetes Care. 2017;40(4):538-545. doi:10.2337/dc16-2482
- Phillip M, Nimri R, Engberg S, et al. Consensus recommendations for the use of automated insulin delivery technologies in clinical practice. Lancet Diabetes Endocrinol. 2023;11(10):766-781. doi:10.1016/S2213-8587(23)00185-8