
The Warsaw Formula for Insulin Dosing: Why Fat and Protein Matter Beyond Carb Counting
For decades, carbohydrate counting has been the gold standard for mealtime insulin dosing in type 1 diabetes. But anyone who has bolused correctly for a pizza and still woken up with a blood sugar of 250 mg/dL knows the system is incomplete. The Warsaw Pump Therapy School developed a formula that accounts for fat and protein—and the evidence suggests it works.
The Pizza Problem: Why Carb Counting Alone Fails
Ask any person with type 1 diabetes what their most difficult meal is, and you will hear the same answers: pizza, takeaway curry, a cheeseburger with fries. These meals share a common trait—they are high in both fat and protein alongside carbohydrates—and they reliably produce a prolonged hyperglycemic excursion that begins 3–5 hours after eating, long after the rapid-acting insulin bolus has finished working.
This phenomenon is not a failure of willpower or counting skill. It is a failure of the model. Standard carbohydrate counting assumes that only carbohydrates meaningfully affect postprandial blood glucose. Clinical evidence has thoroughly disproven this assumption.
Bell et al. (2015) demonstrated in a systematic review that the addition of fat to a meal significantly increases the glycemic excursion at 3–5 hours post-meal, even when carbohydrate content is held constant. The mechanisms are multifactorial: dietary fat slows gastric emptying, delays carbohydrate absorption into a longer and flatter curve, and—crucially—induces hepatic insulin resistance through free fatty acid oxidation. Protein, through gluconeogenesis, provides an additional substrate for endogenous glucose production over 3–8 hours.
The net effect is that a meal containing 80 g of carbohydrate, 40 g of fat, and 35 g of protein requires substantially more insulin—delivered over a substantially longer period—than a meal of 80 g of carbohydrate alone. Carb counting addresses only the first variable.
The Warsaw Pump Therapy School Formula
Researchers at the Department of Paediatrics, Warsaw Medical University, led by Dr. Ewa Pankowska, proposed a systematic method to quantify the insulin required for fat and protein. First described in 2009 and refined in subsequent publications, the approach introduces the concept of the Fat-Protein Unit (FPU).
Defining the Fat-Protein Unit
One FPU is defined as 100 kilocalories derived from fat and protein in a meal. The calculation proceeds as follows:
- Determine the grams of protein and fat in the meal
- Calculate total energy from fat and protein: (protein grams × 4 kcal/g) + (fat grams × 9 kcal/g)
- Divide total energy by 100 to obtain the FPU count
From FPU to Insulin Dose
The Warsaw formula establishes that each FPU has an equivalent glycemic impact to approximately 10 grams of carbohydrate. The additional insulin required is therefore:
Additional insulin = (FPU × 10) ÷ ICR
Where ICR is the individual’s insulin-to-carbohydrate ratio. This additional insulin is delivered as an extended (square-wave) or dual-wave bolus on an insulin pump, or through a delayed injection for MDI users.
Duration of Extended Bolus
The duration over which the additional insulin is delivered depends on the FPU count, reflecting the prolonged digestion time of high-fat, high-protein meals:
1 FPU
3 hours extended bolus duration
2 FPU
4 hours extended bolus duration
3 FPU
5 hours extended bolus duration
4+ FPU
8 hours extended bolus duration
Clinical Evidence: What the Studies Show
The Warsaw formula is not a theoretical construct—it has been evaluated in multiple clinical studies with meaningful results, though not without important caveats.
Pankowska et al. (2009): The Foundational Study
In a study of children with type 1 diabetes using insulin pumps, Pankowska and colleagues demonstrated that application of the dual-wave bolus based on fat-protein content produced a statistically significant reduction in glycated hemoglobin (HbA1c) compared to conventional carbohydrate-only dosing. The study established that accounting for fat and protein reduced late postprandial hyperglycemia—defined as glucose elevation occurring 3–6 hours after the meal—without increasing overall daily insulin by a clinically dangerous amount (Pankowska et al., 2009).
Pankowska & Blazik (2010): Software Implementation
A subsequent paper described the integration of the FPU concept into a bolus calculator with a nutrition database, enabling automated computation of the fat-protein insulin requirement alongside the standard carbohydrate dose. This work demonstrated that the complexity of the calculation need not be a barrier to clinical use if appropriate decision-support tools are available (Pankowska & Blazik, 2010).
Kordonouri et al. (2012): Independent Confirmation
A German randomized controlled trial by Kordonouri and colleagues at Kinderkrankenhaus auf der Bult, Hannover, independently confirmed the benefit of supplementary fat-plus-protein counting. In this study, children with type 1 diabetes on insulin pump therapy were randomized to either conventional carbohydrate counting or carbohydrate counting supplemented by the Warsaw FPU method. The primary outcome was postprandial glucose following a standardized pizza meal.
The results were clear: children using the FPU-supplemented approach had significantly lower blood glucose at the 4–6 hour postprandial time points compared to the carbohydrate-only group. Mean glucose at 6 hours was approximately 40 mg/dL lower in the intervention group—a clinically meaningful difference (Kordonouri et al., 2012).
The Hypoglycemia Caveat
Crucially, several studies have reported an increased risk of early postprandial hypoglycemia when the Warsaw formula is applied. The mechanism is straightforward: fat-induced delayed gastric emptying means the carbohydrate bolus arrives in the bloodstream before the carbohydrate itself is fully absorbed. This creates a mismatch between insulin activity and glucose availability in the 1–2 hour window after the meal.
Kaya et al. documented that when only the insulin-to-carbohydrate ratio was used (without fat-protein adjustment), blood glucose was significantly higher at 120–240 minutes post-meal. However, when the full FPU dose was applied as recommended, early-phase glucose dropped excessively in some patients. This finding reinforces that the Warsaw formula is not a universal “set and forget” solution—it requires individualization, monitoring, and ideally continuous glucose monitoring (CGM) to detect and mitigate early lows.
The Sieradzki Equation: A Simpler Alternative
For clinicians and patients who find the FPU calculation burdensome or who experience unacceptable early hypoglycemia with the full Warsaw approach, the Sieradzki equation offers a pragmatic simplification.
The principle is straightforward: for meals that are high in fat and protein, add 30% of the calculated carbohydrate-based insulin dose as an extended bolus delivered over 2–3 hours.
For example, if the carbohydrate content of a meal requires 6 units of insulin, the Sieradzki approach would add 1.8 units (30% of 6) as a square-wave or extended delivery. This is simpler to calculate mentally, does not require detailed macronutrient analysis, and in some observational studies has shown a lower rate of early hypoglycemic events compared to the full FPU method.
The trade-off is precision. The Sieradzki equation does not differentiate between a meal with 20 g of fat versus 60 g of fat—both receive the same 30% supplement. For many meals this approximation is sufficient; for extreme fat loads (such as a deep-fried meal or a cheese-heavy pizza), the full Warsaw calculation may provide better late-phase coverage.
Warsaw Formula (Pankowska)
- Precise, macronutrient-specific calculation
- Requires detailed fat and protein data
- Variable duration (3–8 hours) based on FPU count
- Better for very high-fat meals
- Higher early hypoglycemia risk
Sieradzki Equation
- Simple 30% rule applied to carb bolus
- Only requires knowledge that meal is high-fat
- Fixed 2–3 hour extended bolus
- Lower cognitive burden
- Potentially fewer early hypo events
Why GlucIQ’s Approach Matters
GlucIQ does not implement the Warsaw formula as an automated dosing system. This is a deliberate design decision rooted in patient safety and clinical appropriateness.
The Warsaw formula requires individualized parameters (ICR, insulin sensitivity factor, pump capabilities) that vary between patients and change over time. Applying it autonomously without clinician oversight introduces risk—particularly the early hypoglycemia risk documented in the literature. No app should unilaterally tell a user “take X units of additional insulin” without the context of their full clinical picture.
What GlucIQ provides instead is the contextual foundation that makes informed decision-making possible:
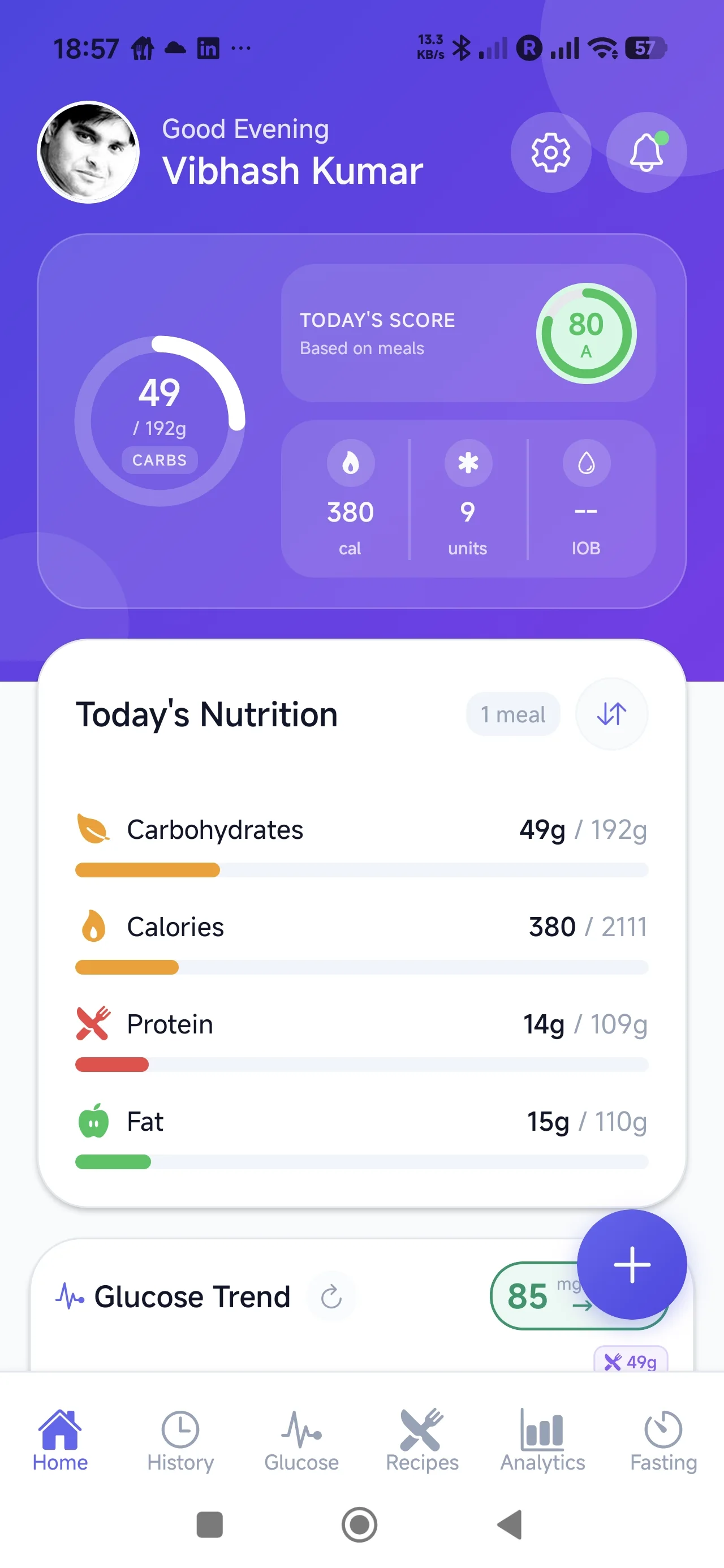
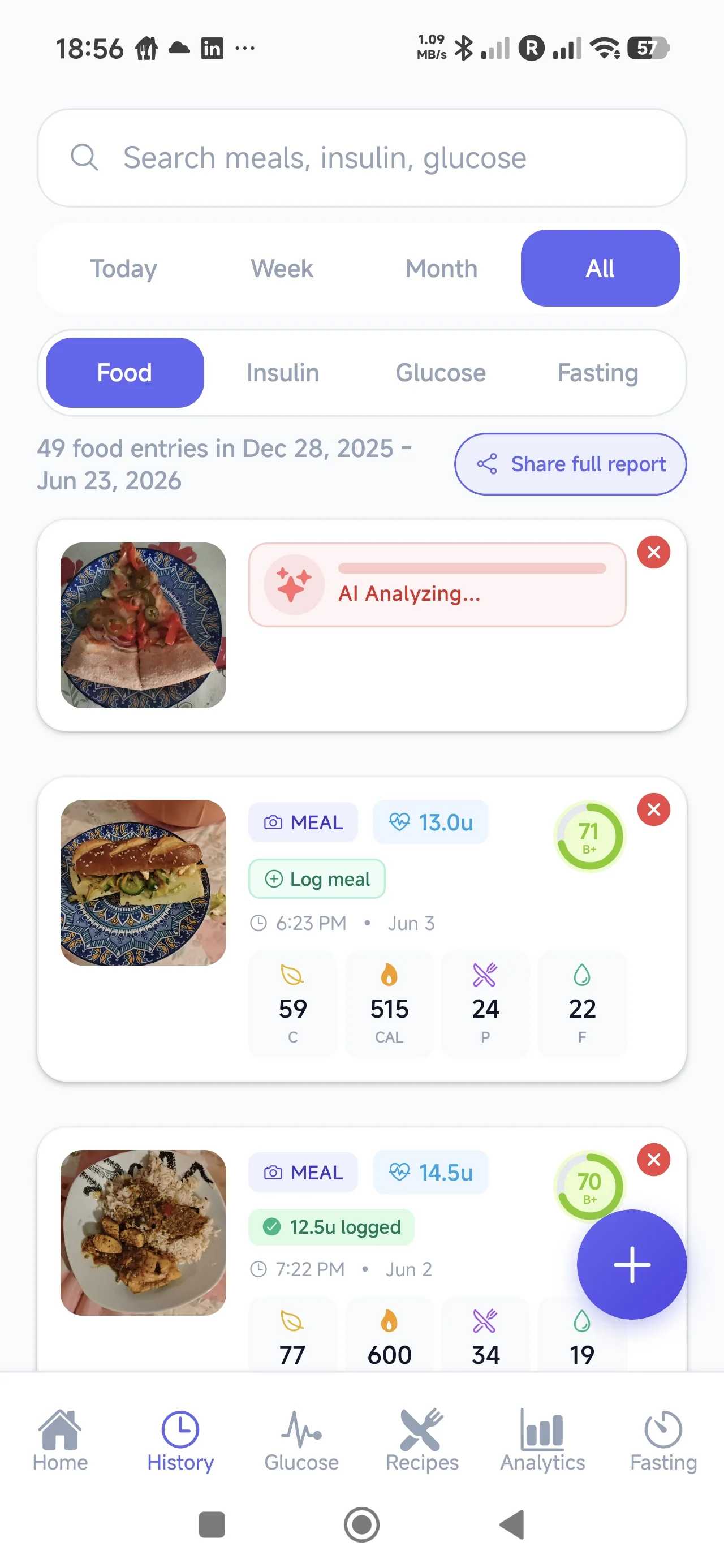
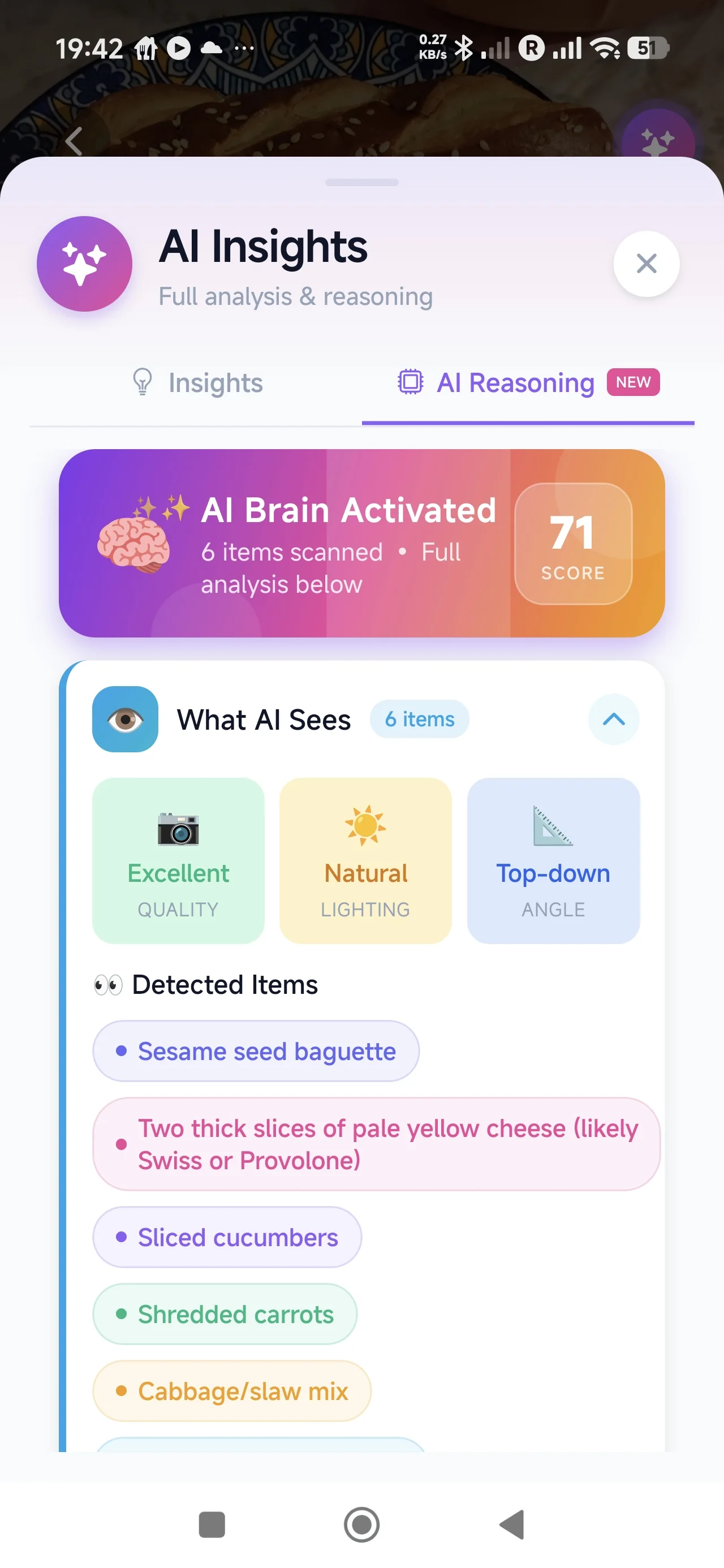
- Detailed meal composition: AI-powered food scanning estimates not just carbohydrates but also fat and protein content, providing the raw data needed for FPU-aware decisions
- Insulin decision logging: Users record what insulin they took and when, creating a complete picture of the dose-response relationship
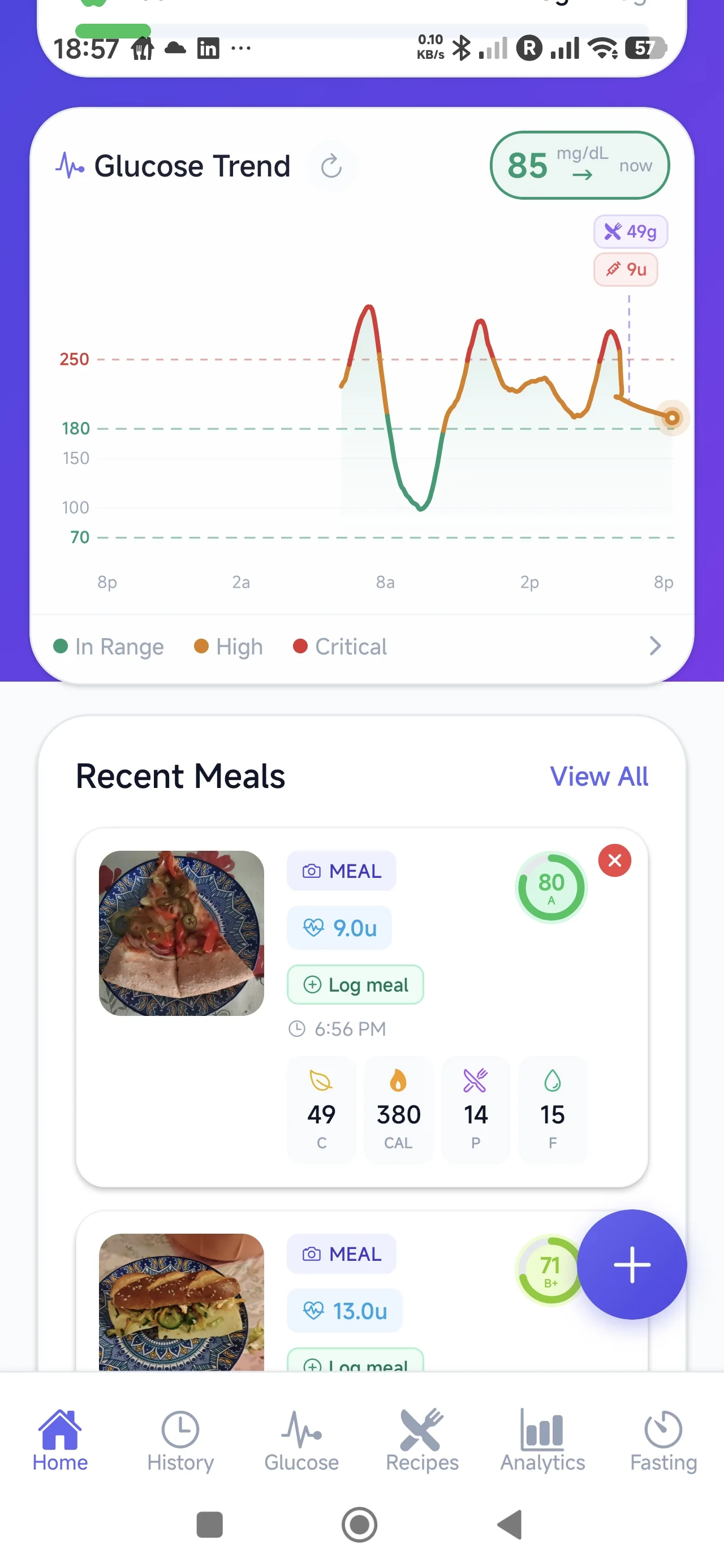
- Glucose response patterns: By capturing glucose data alongside meals and insulin, GlucIQ reveals the 3–6 hour postprandial patterns that indicate whether fat-protein coverage is adequate
- Clinician review capability: The collected data enables healthcare providers to identify patients who may benefit from FPU-based adjustments and to titrate those adjustments safely over time
This philosophy—providing context for decisions rather than making decisions autonomously—respects the complexity of diabetes management and the irreplaceable role of clinical judgment.
Worked Example: Pizza Night
The following example is purely educational and demonstrates how the Warsaw formula calculation works in principle. It is not a recommendation for any individual. All insulin dosing decisions must be made in consultation with your diabetes care team.
The Meal
Two slices of pepperoni pizza (thick crust, from a typical chain):
- Carbohydrates: 62 g
- Protein: 28 g
- Fat: 24 g
Step 1: Standard Carbohydrate Bolus
Assuming an ICR of 1:10 (1 unit per 10 g carbohydrate):
Carb bolus = 62 ÷ 10 = 6.2 units (delivered as normal/immediate bolus)
Step 2: Calculate Fat-Protein Energy
Total kcal from fat and protein:
(28 g protein × 4 kcal/g) + (24 g fat × 9 kcal/g) = 112 + 216 = 328 kcal
Step 3: Determine FPU Count
328 kcal ÷ 100 = 3.28 FPU (round to 3 FPU for duration lookup)
Step 4: Calculate Additional Insulin
Carbohydrate equivalent = 3.28 FPU × 10 g = 32.8 g equivalent
Additional insulin = 32.8 ÷ 10 (ICR) = 3.3 units
Step 5: Determine Delivery Duration
At 3 FPU, the duration table indicates 5 hours of extended bolus delivery.
Summary
Total insulin: 6.2 units immediate + 3.3 units over 5 hours = 9.5 units total
Compare to carb-only: 6.2 units immediate—leaving the 3–6 hour window uncovered.
The Future: AI-Powered Macronutrient Estimation
One of the historical barriers to widespread adoption of the Warsaw formula has been the cognitive burden of calculating fat and protein content for every meal. Carbohydrate counting is already demanding; adding two more macronutrients to track multiplies the effort significantly.
This is where modern computer vision and AI food analysis become transformative. By scanning a meal with a smartphone camera, AI systems can estimate not only carbohydrate content but also fat and protein—the exact inputs required for FPU calculation. What was once a 3-minute mental math exercise becomes a 5-second photo.
GlucIQ’s AI food scanning is designed with this future in mind. By providing comprehensive macronutrient estimates automatically, the app removes the friction that has prevented broader use of fat-protein-aware insulin strategies. The data becomes available; the clinical decision about whether and how to use it remains with the user and their healthcare team.
As continuous glucose monitoring becomes more prevalent and predictive algorithms improve, the combination of accurate meal composition data and real-time glucose feedback creates the conditions for genuinely personalized diabetes management—where the “right” insulin strategy for a given meal can be learned from an individual’s own historical patterns rather than applied from a population-level formula.
Conclusion
The Warsaw formula represents an important advance in our understanding of mealtime insulin dosing. By quantifying the glycemic impact of fat and protein through the Fat-Protein Unit, it provides a systematic framework for addressing the “unexplained” hyperglycemia that follows high-fat meals—the pizza problem that frustrates so many people with type 1 diabetes.
The clinical evidence supports its efficacy in reducing late postprandial hyperglycemia, though the documented risk of early hypoglycemia demands that it be implemented carefully, ideally with CGM and under clinical supervision. The Sieradzki equation offers a simpler alternative for those who need a less computationally intensive approach.
Tools like GlucIQ contribute to this ecosystem not by automating the formula, but by making the underlying data accessible: meal composition, insulin decisions, and glucose response patterns. When users and clinicians can review this data together, the path to personalized fat-protein dosing strategies becomes clearer and safer.
The era of carb-only counting is ending. Fat and protein matter. The question is no longer whether to account for them, but how to do so safely and sustainably in daily life.
Understand Your Meals. Review Your Patterns. Own Your Data.
GlucIQ gives you the full picture—macronutrients, insulin decisions, and glucose responses—so you and your care team can make informed decisions about fat-protein dosing strategies.
References
- Pankowska E, Szypowska A, Lipka M, Szpotańska M, Błazik M, Groele L. Application of novel dual wave meal bolus and its impact on glycated hemoglobin A1c in children with type 1 diabetes. Pediatr Diabetes. 2009;10(5):298–303. doi:10.1111/j.1399-5448.2008.00471.x
- Pankowska E, Blazik M. Bolus calculator with nutrition database software, a new concept of prandial insulin programming for pump users. J Diabetes Sci Technol. 2010;4(3):571–576. doi:10.1177/193229681000400310
- Kordonouri O, Hartmann R, Remus K, Datz N, Klüver IB, Lange K. Benefit of supplementary fat plus protein counting as compared with conventional carbohydrate counting for insulin bolus calculation in children with pump therapy. Pediatr Diabetes. 2012;13(7):540–544. doi:10.1111/j.1399-5448.2012.00880.x
- Bell KJ, Smart CE, Steil GM, Brand-Miller JC, King B, Wolpert HA. Impact of fat, protein, and glycemic index on postprandial glucose control in type 1 diabetes: implications for intensive diabetes management in the continuous glucose monitoring era. Diabetes Care. 2015;38(6):1008–1015. doi:10.2337/dc15-0100